


The last few years has seen a welcome shift by government to addressing the needs of poor and vulnerable households in Pakistan. In 2018-2019, it was estimated that 52% of the entire population of Pakistan was vulnerable to falling back into poverty (Jamal 2021). To further understanding in this area, we conducted research on the needs of vulnerable households from both an environmental and a gender standpoint. What we found (and did not find) provides much insight for change.
This article briefly summarizes our main findings. The second and third articles will propose a way forward to address current issues in a way that benefits the poor and vulnerable, as well as the entire population, reaping multiple co-benefits. The main report is available on the IGC website at: https://www.theigc.org/project/kamyab-pakistan-programme-making-it-green-and-gender-inclusive/
Health and the Environment
The Global Burden of Disease (GBD) study, conducted every 10 years, assesses the major causes of disease that lead to early mortality and high morbidity. The burden of disease attributable to various risk factors is measured in terms of lost years of healthy life using the disability-adjusted life year (DALY) metric. DALY combines years of life lost because of premature death with years of unhealthy life due to illness and disability.
The GBD’s approach is particularly instructive in terms of broader healthcare policy, as it moves away from single disease “silos” to take a wider perspective. Figures 1 and 2 below show the top ten causes of death and of death and disability combined in Pakistan, including the relative increase in these diseases between 2009 and 2019 (GBD 2021). Note the significant increase in ischemic heart disease and stroke, as well as diabetes and kidney diseases in Figure 2. This has shifted the health burden from mainly communicable diseases to a mixture of about 60% non-communicable disease (NCDs) and 40% communicable diseases (CDs) in Pakistan. Unlike CDs, which can be cured, NCDs need to either be prevented or managed throughout a lifetime, resulting in increasing health costs.
Figure 1. What causes the most deaths in Pakistan?
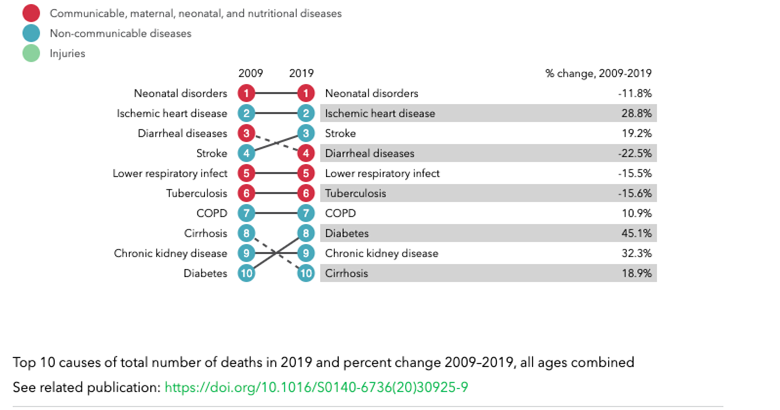
Source: https://www.healthdata.org/pakistan
Figure 2. What causes the most death and disability combined in Pakistan?
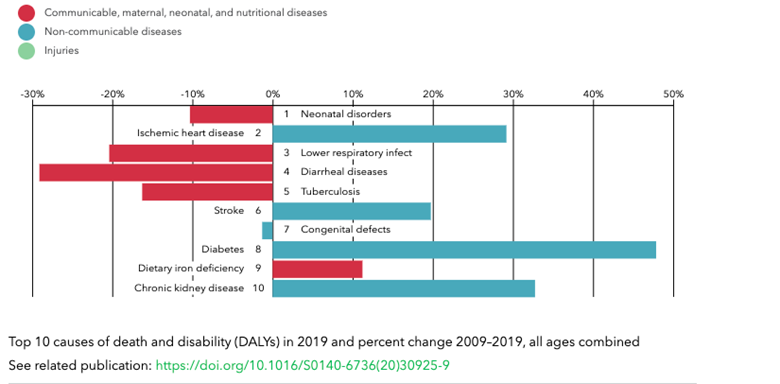
Source: https://www.healthdata.org/pakistan
Figure 3 below shows the major risk factors that drive the most deaths and disability combined for Pakistan in 2019, before the Covid-19 pandemic, compared with 2009. As can be seen, malnutrition occupies the top spot, with air pollution at number 2, consistently, during the 10-year period. Despite some reduction in water, sanitation, hygiene (WaSH) and tobacco related risk, both still appear in the top 10 risks.
Figure 3. What risk factors drive the disease burden (death and disability combined) in Pakistan?
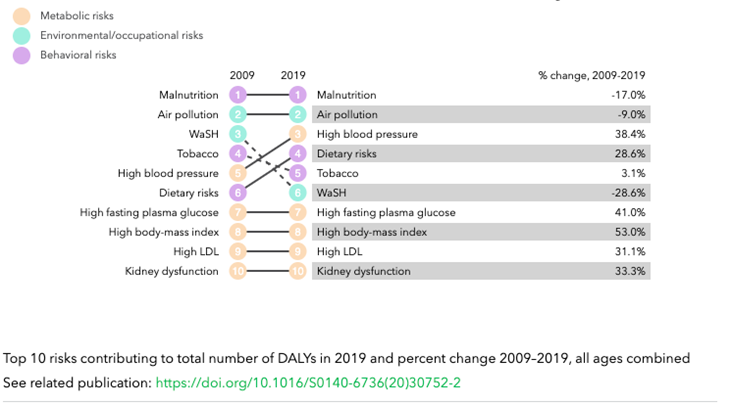
Source: https://www.healthdata.org/pakistan
Air Pollution, Health and Human Capital
The direct health effects of air pollution are well documented. We now have indisputable lab and field evidence that exposure to poor air quality raises the incidence of ischemic heart disease, stroke, lung cancer, neonatal morbidity, lower respiratory infections, diabetes, and chronic obstructive pulmonary disease.
Besides health, air pollution affects human capital, leading to economic and productivity losses. Pollution can directly affect the brain’s neurological function, diminishing cognitive ability. On the other hand, severe morbidities—such as reduced lung function—could reduce one’s focus and hence the ability to perform a range of physical and cognitive tasks. Pollution can therefore increase school and job absences and performance, inhibiting human capital growth and economic productivity.
There is strong evidence that an increase in carbon monoxide levels leads to higher school absences, even when levels lie below mandated standards (Currie et al. 2009). Similarly, improvements in air quality owing to source closures improves school attendance (Pope 1989; Ransom and Pope 1992). Pollution exposure also reduces students’ ability to concentrate and affects brain development (Block and Calderón-Garcidueñas 2009). A longitudinal study from California has shown that a 10 percent decrease in PM2.5 raises school children’s math and reading test scores by 0.14 percent and 0.21 percent, respectively (Zweig, Ham, and Avol 2009). Research in Israel shows that a 10 unit increase in PM2.5 reduces high school students’ test scores by 1.9 percent of a standard deviation while a 10 unit increase in carbon monoxide reduces test scores by 2.4 percent of a standard deviation (Lavy, Ebenstein, and Roth 2012). Both these settings have considerably better air quality than Pakistan.
Exposure to air pollution during gestation can affect children’s human capital outcomes later in life. These include lower scores on language and math tests in school (Bharadwaj et al. 2017); depressed earnings later in life (Isen et al. 2017; Voorheis 2017); high unemployment (Isen et al. 2017); lower probability of college attendance (Colmer and Voorheis 2020); reduced high school completion (Voorheis 2017); and higher chances of incarceration (Voorheis 2017).
Another area of concern—which often goes neglected, and where research is scant in Pakistan—is indoor air pollution (IAP), which results from cooking and heating with solid fuels on open fires and traditional cookstoves. Since women mostly carry the burden of cooking and their children often spend time with them, IAP disproportionately affects women and children. According to the Pakistan Social and Living Standards Measurement (PSLM) survey 2019-2020, only 37% of households have access to clean fuel technology for cooking and lighting. Burning solid fuels can lead to indoor pollution levels that are orders of magnitude higher than outdoor levels. Strong evidence links IAP to acute lower respiratory infections, chronic obstructive pulmonary disease, lung cancer, and increased risk of other morbidities including low birth weight, asthma, tuberculosis, blindness, and cardiovascular diseases.
The Health Burden of the Poor
The poor are disproportionately affected as they do not have the resources to privately ensure that the poor quality of public services is compensated for, such as by buying clean drinking water or sleeping in a room with an air purifier. However, there is a second burden borne by the poor. Their savings or income is diverted towards paying healthcare costs, thus often pulling back the household into poverty. A recent study from China analyzed these linkages between health, income and poverty, noting that illness is the main root of poverty in most low-income groups in rural China (Zhou et al. 2020).
However, there is very poor data available on the burden of disease of the poor in Pakistan. Standard surveys (PSLM, HIES, DHS) also do not make the link between income and health burden. Only anecdotal information is available. For example, during the launch of the Kamyab Pakistan Program, the Prime Minister and Finance Minister both directly indicated that health impacts were a major drain on resources for poor and vulnerable households, hence putting in place a health insurance scheme, through the Sehat card, to help with management of health shocks in the short term.
This very clear shortcoming with respect to data collection needs to be addressed, so policymakers are more aware of the situation on the ground and can also monitor any improvements over time based on policies promulgated.
The only exception appears to be data on children under 5 years of age. Infant and child mortality rates vary by income quintile, as can be seen in Figure 4 below. The number one killer of children in Pakistan today is pneumonia and the number two killer is diarrhea. Deaths from pneumonia and diarrhea are also correlated with income quintile in Pakistan (Chang et al. 2018). Environmental risk factors (namely, air and water pollution) play a major role in increasing susceptibility of children to these diseases. The fact that such deaths are higher for lower income quintiles suggests that these income groups face greater exposure to environmental risk factors. A multidimensional approach to addressing these illnesses would also include tackling environmental risk factors.
Figure 4. Mortality and Stunting rates for Pakistani Children
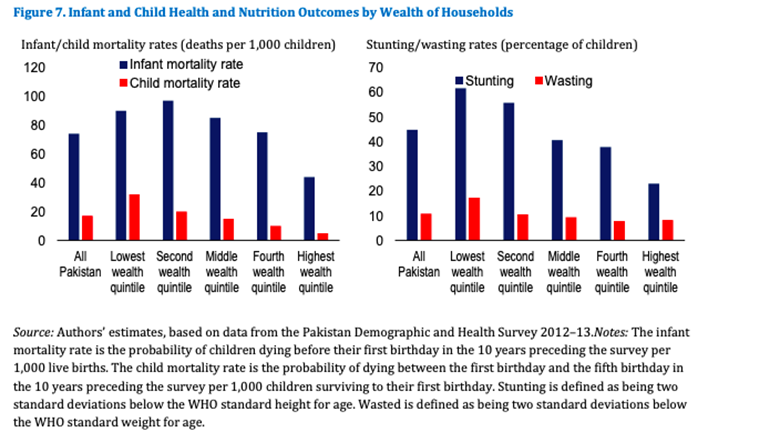
Source: Ahmed et al, 2019.
The children of the poor also suffer the most with respect to stunting and wasting: in Pakistan, 57% of children under the age of 5 years are physically stunted in the lowest income quintile compared with 22% in the highest income quintile. Stunting is typically the outcome of malnutrition. Some malnutrition arises from lack of food and some from the inability to fully benefit from the nutrients in food due to (lower) respiratory infections or diarrhea, both often caused by exposure to polluted air and water. For higher income quintiles, one does not expect stunting due to lack of food, and therefore much of this stunting is probably due solely to environmental risk factors. Since the poor are even more exposed to these same environmental risk factors, one would expect the contribution from environmental risk factors to be even higher.
Figure 5: Stunting in Pakistani Children by Household Wealth
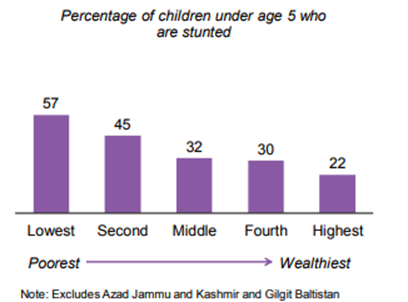
Source: Pakistan DHS 2017-18
Gender, Productivity, and the Poor
With only half of the working age population at work, our nation of 200 million relies on the income of 46 million earners, with each earner supporting 4 dependents on average (Cho and Majoka, 2020). Diversifying household income via multiple earners has increasingly become the norm across many countries as it reduces vulnerability coming from precarious employment and low pay. In Malaysia, female employment has consistently grown in the last five decades, following a concerted policy effort for the development of women in the 1990s. This has in turn led to an increase in dual-income families in the country (Zaimah et al. 2013).
In Pakistan, nearly a third (33.75%) of households have more than one income earner, of which nearly half (43%) have at least one earning woman. Multiple-earner households report a significantly higher monthly income: an average of PKR 34,000 compared to PKR 14,000 earned by single earner families. Multiple-earner households where women also work earn PKR 5,000 more than single-earner families (PSLM 2019-2020, based on author’s calculations). This may be because women tend to engage in informal, often low-pay, work, and may not be compensated at the same rate as men.
Compared to single earner households, multiple earner households where at least one of the earners is a female are, on average, 7 percentage points more likely to have worried about not having enough food to eat; 10 percentage points more likely to have experienced a time when they were unable to eat healthy and nutritious food; and 10 percentage points more likely to have lacked food diversity because of lack of money/ resources in the last 12 months. This suggests that women are working primarily to augment income in vulnerable households. Indeed, female labor force participation is the highest among low income quartiles (24%), falling by a third for the highest income quartile (see Figure 6 below). As can also be seen below, while labor force participation for men is consistently high among all income groups, labor force participation by women is substantially lower at all levels, and decreases with income.
Figure 6. Female Participation by Income Quintile
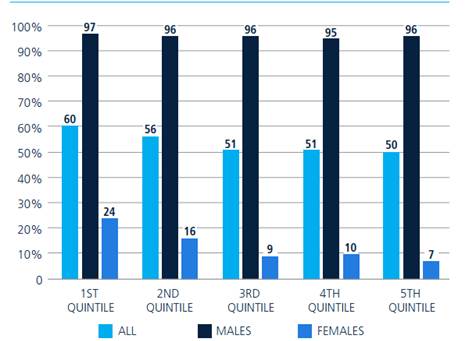
Notes: The graph plots female labor force on the y-axis and income quintiles, disaggregated by gender, on the x-axis.
Source: Cho and Majoka (2020)
Female labor force participation in Pakistan is among the lowest in South Asian countries and stagnant at under 30%. This is particularly true in urban areas, where female labor force participation has been hovering around 11% during 2001-2017 (Cho and Majoka 2020) and holds even among educated graduates (at 25.9%). Women represent a large, untapped productive resource of the country. According to one estimate, closing the gender gap in labor force participation could lead to a (one-off) 30% boost in GDP (Cuberes and Teignier 2014).
Figure 7. GDP losses due to economic gender gaps in selected countries
Source: Cuberes and Teignier (2014). Losses are estimates for a particular year for each country and can be interpreted as a one-off increase in GDP (%) if gender gaps were removed.
Female employment has proven welfare impacts, both for the women themselves and for their dependents. For instance, women who work in Pakistan are more likely to have a say in household consumption decisions and their own health decisions, including the decision to use contraception (Fatima 2014). Similarly, when women are part of household decision making, households tend to spend more on young girl’s education than the average household, and as much as 13% more than the expenditure on boys (Saleemi and Kofol 2022; Data from Pakistan Rural Household Surveys 2014, 2016, 2017). A recent evaluation of Benazir Income Support Programme (BISP), the federal social safety net program, indicates that the periodic unconditional grants, given to women, led to substantial decrease in child labor in the household, with greater decrease in hours worked for girls than for boys (Churchill 2021). This and other international evidenceon the welfare impacts of female employment and decision-making power stresses the importance of including women for sustained growth and prosperity of vulnerable low-income households (Duflo 2003, Chattopadhyay and Duflo 2004, Duflo and Udry 2004).
Research suggests that major challenges to women’s participation in the Pakistani workforce include: (i) financial exclusion and lack of access to finance; (ii) inadequate skills, including low digital literacy; and (iii) lack of safe transport options. The overarching constraint appears to be social norms. Women usually require permission to work from other household members (including to leave the home). Some work is also considered inappropriate or unsafe for women.
Changing this mindset will require a concerted push to include women in the workforce at all income levels. The benefits will accrue both nationally, but also disproportionately for vulnerable households to increase their resiliency.
Policy Recommendations
In summary, our findings suggest:
- An understanding of the actual disease burden across the country broken down by income quintile is sorely lacking. Better information will lead to design of more effective public health and economic policies, so that health costs are not just transferred to different stakeholders within the country but actually reduced. Better data collection will also allow monitoring to track impacts of any efforts to change the situation.
- Addressing environmental risk factors will help ameliorate Pakistan’s health burden, disproportionately benefiting the poor. Since air pollution is the second highest risk factor underpinning Pakistan’s health burden and there is already much focus on water and sanitation, we focus on actions to address air pollution in the second article in this series.
- Increasing gender participation in the workforce across all income quintiles could have multiple benefits. These include an increase in overall GDP, welfare improvement for women and dependents including an increase in amounts spent on girls’ education and potentially a shift in the nature of female employment in vulnerable households helping to increase their resiliency. Hence, in the third article, we focus on actions to increase women’s participation in the workforce.
This article has been authored by a team comprising Kulsum Ahmed (Director, Integrated Learning Means (ILM), Fellow Consortium for Development Policy Research (CDPR)), Ijaz Nabi (Chairman, CDPR and Country Director, IGC and former Sector Manager, World Bank), Sanval Nasim (Assistant Professor, Colby College), and Farah Said (Assistant Professor, Lahore University of Management Sciences (LUMS))
References
Ahmed, Syud Amer, Yoonyoung Cho, and Tazeen Fasih. 2019. “Pakistan at 100: Human Capital” World Bank Group.
Alam, Md Ashraful, Stephanie A. Richard, Shah Mohammad Fahim, Mustafa Mahfuz, Baitun Nahar, Subhasish Das, Binod Shrestha et al. 2020. “Impact of early-onset persistent stunting on cognitive development at 5 years of age: Results from a multi-country cohort study.” PloS one 15(1): e0227839.
Bharadwaj, Prashant, Matthew Gibson, Joshua Graff Zivin, and Christopher Neilson. 2017. “Gray matters: Fetal pollution exposure and human capital formation.” Journal of the Association of Environmental and Resource Economists 4(2): 505-542.
Block, Michelle L., and Lilian Calderón-Garcidueñas. 2009. “Air pollution: mechanisms of neuroinflammation and CNS disease.” Trends in neurosciences 32(9): 506-516.
Burkhardt, Jesse, Jude Bayham, Ander Wilson, Ellison Carter, Jesse D. Berman, Katelyn O’Dell, Bonne Ford, Emily V. Fischer, and Jeffrey R. Pierce. 2019. “The effect of pollution on crime: Evidence from data on particulate matter and ozone.” Journal of Environmental Economics and Management 98: 102267.
Chang, Angela Y., Carlos Riumallo-Herl, Joshua A. Salomon, Stephen C. Resch, Logan Brenzel, and Stéphane Verguet. 2018. “Estimating the distribution of morbidity and mortality of childhood diarrhea, measles, and pneumonia by wealth group in low-and middle-income countries.” BMC medicine 16(1): 1-13.
Chattopadhyay, Raghabendra, and Esther Duflo. 2004. “Women as policy makers: Evidence from a randomized policy experiment in India.” Econometrica 72(5): 1409-1443.
Cho, Yoonyoung, and Zaineb Majoka. 2020. Jobs Diagnostic Pakistan: Promoting Access to Quality Jobs for All. World Bank Group.
Churchill, Sefa Awaworyi, Nasir Iqbal, Saima Nawaz, and Siew Ling Yew. 2021. “Unconditional cash transfers, child labour and education: theory and evidence.” Journal of Economic Behavior & Organization 186: 437-457.
Colmer, Jonathan, and John Voorheis. 2020. “The grandkids aren’t alright: the intergenerational effects of prenatal pollution exposure.”
Cuberes, David, and Marc Teignier. 2014. “Gender inequality and economic growth: A critical review.” Journal of International Development 26(2): 260-276.
Currie, Janet, Eric A. Hanushek, E. Megan Kahn, Matthew Neidell, and Steven G. Rivkin. 2009. “Does pollution increase school absences?” The Review of Economics and Statistics 91(4): 682-694.
D’Adda, Giovanna, Mahreen Mahmud, Farah Said, and Diego Ubfal. 2019. “Constraints to female entrepreneurship in Pakistan: The role of women’s goals and aspirations.” International Growth Centre.
Dong, Rui, Raymond Fisman, Yongxiang Wang, and Nianhang Xu. 2021. “Air pollution, affect, and forecasting bias: Evidence from Chinese financial analysts.” Journal of Financial Economics 139(3): 971-984.
Duflo, Esther. 2003. “Grandmothers and granddaughters: old‐age pensions and intrahousehold allocation in South Africa.” The World Bank Economic Review 17(1): 1-25.
Duflo, Esther, and Christopher R. Udry. 2004. “Intrahousehold resource allocation in Cote d’Ivoire: Social norms, separate accounts and consumption choices.”
Fatima, Duryab. 2014. “Education, employment, and women’s say in household decision-making in Pakistan.”
Global Burden of Disease Collaborative Network., 2021. Global Burden of Disease Study 2019 (GBD 2019) Reference Life Table. Seattle, United States of America: Institute for Health Metrics and Evaluation (IHME).
Graff Zivin, Joshua, and Matthew Neidell. 2012. “The impact of pollution on worker productivity.” American Economic Review 102(7): 3652-73.
Hanna, Rema, and Paulina Oliva. 2015. “The effect of pollution on labor supply: Evidence from a natural experiment in Mexico City.” Journal of Public Economics 122: 68-79.
Herrnstadt, Evan, Anthony Heyes, Erich Muehlegger, and Soodeh Saberian. 2021.”Air pollution and criminal activity: Microgeographic evidence from Chicago.” American Economic Journal: Applied Economics 13(4): 70-100.
Huang, Jiekun, Nianhang Xu, and Honghai Yu. 2020. “Pollution and performance: do investors make worse trades on hazy days?.” Management Science 66(10): 4455-4476.
Isen, Adam, Maya Rossin-Slater, and W. Reed Walker. 2017. “Every breath you take—every dollar you’ll make: The long-term consequences of the clean air act of 1970.” Journal of Political Economy 125(3): 848-902.
Jamal, Haroon. 2021. “Updating Pakistan’s Poverty Numbers for the Year 2019.” Social Policy and Development Center (SPDC), Karachi, Pakistan.
Lavy, Victor, Avraham Ebenstein, and Sefi Roth. 2012. “The impact of air pollution on cognitive performance and human capital formation.” Unpublished. http://www2. warwick. ac. uk/fac/soc/economics/staff/academic/lavy/text_and_tables_air_pollution_draft_20_09_12. pdf.
Pope 3rd, C. A. 1989. “Respiratory disease associated with community air pollution and a steel mill, Utah Valley.” American journal of public health 79(5): 623-628.
Ransom, Michael R., and C. Arden Pope III. 1992. “Elementary school absences and PM10 pollution in Utah Valley.” Environmental research 58(1-2): 204-219.
Saleemi, Sundus, and Chiara Kofol. 2022. “Women’s participation in household decisions and gender equality in children’s education: Evidence from rural households in Pakistan.” World Development Perspectives 25: 100395.
Sokolovic, N., S. Selvam, K. Srinivasan, P. Thankachan, A. V. Kurpad, and T. Thomas. 2014. “Catch-up growth does not associate with cognitive development in Indian school-age children.” European journal of clinical nutrition 68(1): 14-18.
Voorheis, John. 2017. “Air quality, human capital formation and the long-term effects of environmental inequality at birth.” US Census Center for Economic Studies, CARRA Working Paper Series 5.
World Bank. 2008. Environmental health and child survival: epidemiology, economics, experiences. The World Bank.
World Health Organization. 2021. Household Air Pollution and Health, Fact Sheet, 22 September 2021. https://www.who.int/news-room/fact-sheets/detail/household-air-pollution-and-health
Zaimah, R., M. S. Sarmila, S. Selvadurai, N. Lyndon, A. C. Er, and Muhd Norizam Jamian. 2013. “The history and current status of dual-career families in Malaysia.” Asian Social Science 9(6): 16.
Zhou, Yang, Yuanzhi Guo, and Yansui Liu. 2020. “Health, income and poverty: Evidence from China’s rural household survey.” International Journal for Equity in Health 19(1): 1-12.
Zweig, Jacqueline S., John C. Ham, and Edward L. Avol. 2009. “Air pollution and academic performance: Evidence from California schools.” National Institute of Environmental Health Sciences: 1-35.


